Max Rady College of Medicine
Concept: Intra-Urban Areas
Concept Description
Last Updated: 2008-05-26
Background Information
-
The information in this concept is based on work by
DeVerteuil, G. et al.
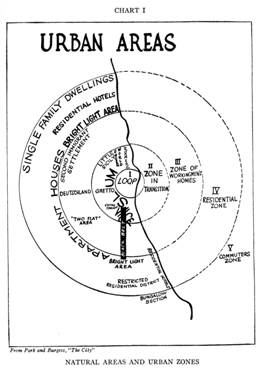
A traditional task in urban geography has been to "conceptually understand how urban society is organized spatially, a perspective we now call spatial or urban ecology" (Kaplan et al., 2004) . Beginning with the Chicago School of Urban Sociology in the 1920s, the spatial organization of urban society has been tied to identifying and differentiating areas within cities ( intra-urban zones ) that encompass distinct physical and social characteristics. The famous Burgess concentric zone model differentiated a number of intra-urban areas, beginning at the center with the Central Business District (CBD or "downtown"), and moving outward (and socio-economically upward) through the zone in transition, the zone of workingmen's homes, the residential zone, and finally the commuters' zone. Each of these intra-urban zones represented the outcomes of invasion and succession of different socio-economic and ethnic groups, as they sought out particular "niches" that maximized social and spatial distance from competing groups.
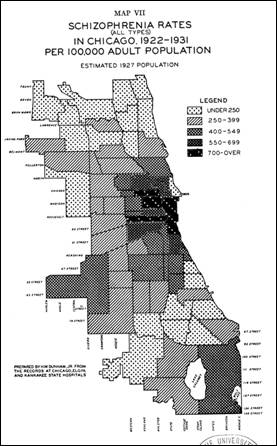
Of all the Burgess zones, it was the inner city - roughly equivalent to the zone of transition - that attracted the most academic attention, given the persistent pooling of social pathologies (crime, vice, poverty, gangs, etc.) in this intra-urban area. This focus has also extended to health geography. In their classic study on the geographic variability of mental illness in the city, Faris and Dunham (1939) observed an association between high rates of certain severe mental illness (SMI) - such as schizophrenia - and residence in disadvantaged, socially disorganized inner-city neighbourhoods in Chicago.
The images below show the concentric zone model, and how rates of schizophrenia were strongly associated with Chicago's inner city (from Faris and Dunham, 1939 ).
|
Burgess concentric zone model
|
Chicago Schizophrenia Rates
|
|
|
Steps for Determining Core/Suburban Community Centre Areas
-
For the mental health and mobility study, the specific data and analysis used to define and identify intra-urban areas for the Winnipeg Regional Health Authority (WRHA) are as follows:
Defining Intra-Urban Areas
Three intra-urban areas were chosen, based on urban theory and two previous Canadian studies (see McLemore, Aass, and Keilhofer, 1975 ; Ram, Norris, and Skof, 1989 ) that took the "inner city" (but not any other areas) as those neighborhoods in proximity to the CBD with substantial pre-1946 housing stock.
With this background in mind, we conceptualized the inner core to correspond to the disadvantaged, heterogeneous "zone of transition" in the Chicago model: the oldest, densest and poorest areas of Winnipeg.
We conceptualized the outer core to correspond to the oldest and densest areas of the city, but not the poorest. These neighborhoods tend to be elite areas that have maintained their social and physical integrity (see Ley, 2001 ).
Finally, the suburb is basically the remaining areas of the city - by default, the newest, least dense areas.Methodology
Data for the intra-urban analysis was based on 2001 Canadian Census Data at the dissemination area and Community Centre Area for the WRHA. Data was extracted from 2001 census on housing age (total number of occupied private dwellings, construction pre-1946), density (population, CCA area in hectares), and income (median 2000 household income; incidence of low income among economic families).
Below are the specific steps to designate the inner core, outer core and suburbs.
- Assign the Census 2001 dissemination areas to the 75 community centre areas, using a conversion table provided by the MCHP, in order to aggregate dissemination area data from the 2001 Census to the appropriate CCA.
- Once the population-weighted dissemination data have been aggregated by CCA, it was possible to calculate for each CCA its density (population divided by hectare), the proportion of housing stock built before 1946 (pre-1946 stock divided by entire occupied housing stock), and the median household income. Using population-weighted CCA values, it was then possible to calculate median values for the entire WRHA for density (23.36 persons per hectare), the proportion of housing stock for each CCA built before 1946 (19.75%), and household income ($46,425).
- Using the query builder in ArcView, find all CCAs that had above median density and median pre-1946 construction - this represents the core area (both inner and outer).
- Include contiguous CCAs to the inner core (i.e. downtown, etc.). Note that the following rules are sequential.
- RULE 1: The Ram, Norris and Skof (1989) study on the Canadian inner-city identified two more CCAs - 73 (Downtown) and 8 (Central)- that belong in the inner core. The study determined inner-city boundaries by "land use and age of development criteria, selected in consultation with the Planning Departments of respective cities. Thus, the inner city refers to the core of the metropolitan area, which includes the site of the earliest development of the city, the Central Business District (CBD) , and the surrounding areas of mixed land uses, with high density residential development". 29 CCAs were assigned to the inner core by this rule.
- RULE 2: Contiguity rule was applied to remaining CCAs with either above average density and above median pre-1946 housing stock, and that the remaining CCAs had to have at least half their borders with core CCAs (n=4). This rule was applied only once, and did not consider areas that were contiguous after the subsequent CCAs were chosen.
There is now a total of 33 CCAs.
- RULE 3: Of the core CCAs with less than the median of the median household incomes ($46,425) for all the CCAs, 27 CCAs were considered "inner core areas"; those above the median were considered "outer core areas" (see map ).
All the remaining CCAs were considered suburban.
- As the results below demonstrate, the outer core areas are older and denser than the Winnipeg city median; the inner core areas are older, denser and poorer than the Winnipeg city median; and all other CCAs are by default suburban.
Identifying Winnipeg's Intra-Urban Areas
-
Results for the three areas, using 2001 census data, are tabled below:
Intra-urban area Population Median % pre-1946 (sd) Median household income (sd) Median pop density (sd)
Inner core 189,090 44.8% (15.1) $33,579 (7395) 31.03 (17.01)
Outer core 44,393 40.8% (9.9) $49,152 (12490) 26.95 (7.83)
Suburb 408,107 4.6% (1.2) $59,557 (15937) 18.87 (4.92)
How the three areas are related to mental health services is described below:
Intra-urban area Average Gross Rent in $Cdn Psychiatric beds per 1,000 population a Licensed mental health care facility beds per 1,000 population b Rooming home units per 1,000 population c
Inner Core $ 518.51 0.61 1.39 3.92
Outer Core $ 882.50 0
0.16 0.36
Suburb $ 603.00 0.19 0.24 0.06 Note:
a - Data for psychiatric beds were obtained from the Winnipeg Regional Health Authority (WRHA), December 2000; population data are from the 2001 census.
b - Data for licensed mental health care facilities (which provide space for 4-6 residents) was provided directly by the WRHA, December 2001; population data are from the 2001 census.
c - Rooming home data were obtained from a 1999 City of Winnipeg survey; population data are from the 2001 census.
Mapping Intra-Urban Areas for Winnipeg
-
The three intra-urban areas were mapped for Winnipeg. Not surprisingly, the inner core occupies the inner parts of Winnipeg; the outer core is directly to the south of the inner core; and the suburbs encompass the outlying parts of the city.
Limitations
-
One obvious limitation is that this sort of analysis works best with a monocentric city such as Winnipeg. In polycentric, more complex urban regions such as Los Angeles, it may be very difficult to delineate the inner/outer core from the suburbs.
Related terms
References
- Dear MJ, Bayne L, Boyd G, Callaghan C, Goldstein E. Coping in the Community: The Needs of Ex-Psychiatric Patients. Hamilton, ON: Canadian Mental Health Association; 1980.(View)
- Dear MJ, Wolch JR. Landscapes of Despair: From Deinstitutionalization to Homelesness. Princeton, NJ: Princeton University Press; 1987.(View)
- DeVerteuil G, Hinds A, Lix L, Walker J, Robinson R, Roos L. Mental health and the city: Intra-urban mobility among individuals with schizophrenia. Health & Place 2007;(13(2)):310-323. [Abstract] (View)
- Faris RE, Dunham W. Mental Disorders in Urban Areas: An ecological study of Schizophrenia and other psychoses. Chicago, IL: University of Chicago Press; 1939.(View)
- Giggs JA. The distribution of schizophrenics in Nottingham. Transactions of the Institute of British Geography 1973;59:55-76.(View)
- Kaplan D, Wheeler J, Holloway S. Urban Geography. New York, NY. Wiley Press; 2004.(View)
- Ley D. "The inner city." In: Bunting, T, et. al. (eds). Canadian Cities in Transition. Toronto, ON: Oxford University Press; 2001.(View)
- Lix LM, Hinds A, DeVerteuil G, Robinson JR, Walker J, Roos LL. Residential mobility and severe mental illness: a population-based analysis. Adm Policy Ment Health 2006;33(2):160-171. [Abstract] (View)
- McLemore R, Aass C, Keilhofer P. The Changing Canadian Inner-City. Ottawa, ON: Ministry of State for Urban Affairs; 1975.(View)
- Ram B, Norris M, Skof K. The Inner City in Transition. Ottawa, ON: Minister of Supply and Services Canada; 1989.(View)
- Silver E, Mulvey E, Swanson J. Neighborhood structural characteristics and mental disorder: Faris and Dunham revisited. Social Science and Medicine 2002;55(8):1457-1470.(View)
- Thornicroft G. Social deprivation and rates of treated mental disorder. British Journal of Psychiatry 1991;158:475-484.(View)
- Wolch J, Philo C. From distributions of deviance to definitions of difference: Past and future mental health geographics. Health and Place 2000;6(3):137-157.(View)
Request information in an accessible format
If you require access to our resources in a different format, please contact us:
- by phone at 204-789-3819
- by email at info@cpe.umanitoba.ca
We strive to provide accommodations upon request in a reasonable timeframe.
Contact us
Manitoba Centre for Health Policy
Rady Faculty of Health Sciences,
Room 408-727 McDermot Ave.
University of Manitoba
Winnipeg, MB R3E 3P5 Canada
204-789-3819